
Today, entire neighborhoods are caring for each other. In the wake of the COVID-19 pandemic, mutual aid has proven an effective response, even if it is not ideal. While these efforts are often contextualized within a radical heritage that includes the Black Panther Party’s community programs of the 1960s and 1970s, these genealogies of mutual aid tend to overlook queer care and volunteer responses to AIDS in the 1980s. Looking deeper at that response can shed light on commonalities between the AIDS/HIV and COVID-19 crises, but it also points to a much deeper tradition of the capacity of humans to care for one another, independent of the state (especially when its response has been negligent).


In San Francisco, the HIV and cancer agency Shanti Project has lately reimagined its services to include programs like helping seniors and severely disabled people with their survival needs (and ballots) in the face of COVID. This is not the first time Shanti has altered its service model in the face of crisis. Originally a peer-counseling service for people with terminal diseases, Shanti was one of the first organizations in the U.S. to provide services to people living with AIDS (PWAs), starting in the 1980s. Shanti’s origin is steeped in the tenets of mutual aid, mirroring the way the anarchist Peter Kropotkin conceived it in the nineteenth century. Most established HIV/AIDS organizations are now nonprofits, thus marking them as not “pure” mutual aid, according to academics and activists who comply with the “solidarity not charity” definition of mutual aid.
Weekly Newsletter
The core definition of mutual aid in Kropotkin’s writings, especially Mutual Aid (1902), is that people may give each other what they need to survive without permission from the state. In that book as well as The Conquest of Bread (1892) and Fields, Factories, and Workshops (1898), Kropotkin advanced the idea as the opposite of “survival of the fittest” ideology, used to justify the poverty innate to the expanding industrial revolution and onset of global capitalism. Kropotkin’s alternative visions of local economies and people’s tending to one another’s needs influenced generations of social scientists and activist thinkers. Kropotkin would share his vision through lectures in the United States, including a notable stay at Hull House hosted by Jane Addams, the founder of the settlement house movement.
Although their missions were diverse, both Addams’s Hull House and Catholic Worker “houses of hospitality” provided everyday survival needs and a safe place to meet and rest for impoverished and unhoused individuals who had nowhere else to turn. Most importantly in the movements’ practice, those who received aid and those who provided it were to be close, because this proximity would lead to transformative changes on both sides. The early responses to AIDS show little evidence of being directly influenced by Kropotkin. But the influence of his ideas about mutual aid was present in the emphasis on exchange, especially in Shanti’s work.
Founded in 1974 by Charles Garfield in Berkeley, California, Shanti began by providing intimate peer counseling to enhance the quality of care (and of life) for people with terminal illness and to provide support to their loved ones. Early clients were matched with a volunteer who went through arduous training in active listening and client advocacy. Most clients in the 1970s were cancer patients and their family members. At the dawn of the 1980s, a small number of clients emerged—all gay men, usually white—who had rare forms of cancer. Then executive director Jim Geary received a call from San Francisco-based gay psychotherapist Paul Dague, who was on the faculty of the University of California San Francisco. Dague had seen a growing number of gay men in his office with the visibly startling lesions of Kaposi’s Sarcoma (KS) and had even been hired as support at UCSF’s The Kaposi’s Sarcoma Clinic (referred to as The KS Clinic). He thought these new patients needed more counseling than he could provide. UCSF simply did not have the budget for such a service. Geary and another gay Shanti volunteer, Steve Peskind, who later co-founded the Buddhist AIDS Project, soon organized and facilitated the first known support group for gay men with KS and rare cancers in December of 1981. Dague himself was eventually diagnosed with KS and became a member of this very support group until his death three years later.
The “gay cancer” was finally recognized as AIDS in 1982, but it took two more years until HIV was identified as the virus that caused it. Between 1981 and 1984, attendees of Shanti’s initial KS support groups were some of the earliest gay men to live publicly with their diagnosis. One was Bobbi Campbell, a gay nurse who Dague, through The KS Clinic, put in touch with Geary and Shanti.
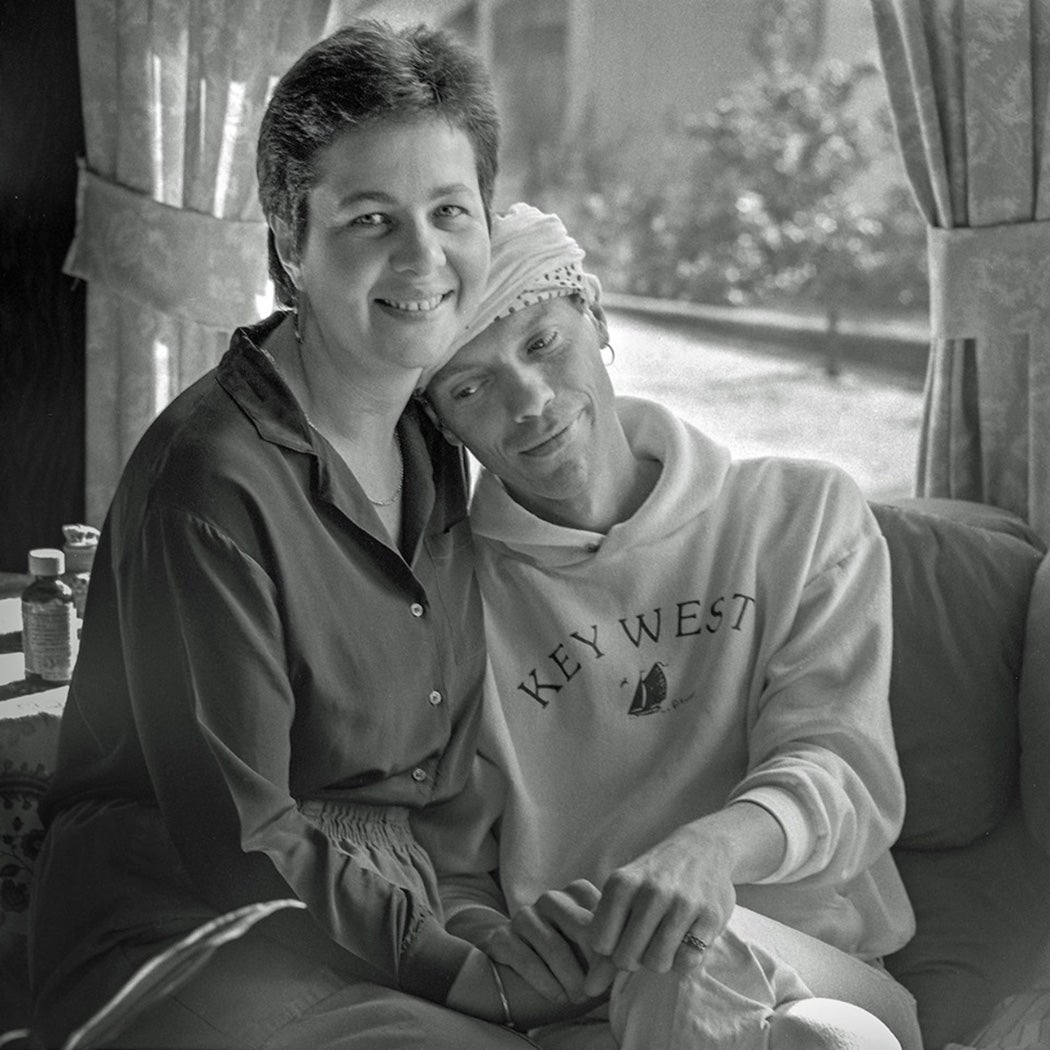
Campbell wrote about the support group in for the local gay newspaper Sentinel, his column was titled the “Gay Cancer Journal.” The Shanti KS support group was incredibly validating for the men in it. Campbell told Sentinel readers, “We form a tight circle and hug each other for several minutes—sometimes we cry. It’s the high point of my week. These men know what I’m going through more than anyone else.” Many of them would hold the iconic banner that proclaimed “Fighting for Our Lives” at the first Candlelight Memorial March in San Francisco in 1983. Shanti nourished this space, created for and, in a way, by them, to provide each other emotional support and validation for their experiences of loss, rage, pain, and sometimes joy.
In PWA support groups momentum grew not only for groundbreaking services to be developed, but also a movement that would write the “Denver Principles.” Shanti support group members Campbell and Bobby Reynolds and PWA activist Dan Turner represented San Francisco in a meeting with other PWAs from across the country at the 1983 the National Gay and Lesbian Health Conference in Denver, Colorado. Together this group crafted The Denver Principles and read them before the entire conference. Opening with the declaration “We condemn attempts to label us as ‘victims,’ which implies defeat, and we are only occasionally ‘patients,’ which implies passivity, helplessness, and dependence upon the care of others. We are ‘people with AIDS.’” The document goes on to list guidelines for healthcare professionals and organizations working with PWAs. This document laid the groundwork for a PWA led movement to take flight in the form of People with AIDS Coalition chapters across the U.S. and later ACT UP.
Shanti relocated from Berkeley to San Francisco in 1982 to better meet the needs of its PWA clients. In 1984, it officially became an AIDS service organization. Volunteer services quickly expanded and separated into the Emotional Support and Practical Support programs. Shanti volunteers sat with clients in their homes or went with them to doctor appointments. Often this interaction made a difference in the quality of the client’s life and in their day to day, if not hour by hour, needs and well-being. Emotional support volunteers would listen and be present for a client—sometimes just chatting or watching television together was enough. Sometimes volunteers and clients would grieve or rage together. For clients who did not want intense counseling, practical support volunteers would do errands, chores, or take part in the van transportation program. They were still prepared to provide more emotional support if it was appropriate. Shanti’s work also extended beyond PWAs’ homes.
Shanti became integral to the “San Francisco model” of AIDS care: a symbiotic relationship between AIDS service organizations, hospitals, research institutions, and social services, to care for PWAs and keep their care affordable and their support systems intact as much as possible. The San Francisco AIDS Foundation provided education and social services and the AIDS Health Project provided clinical psychological care and testing. Shanti took on the psychosocial support for PWAs. Seeping beyond its sole location, Shanti partnered with San Francisco General Hospital’s nurse-managed inpatient AIDS unit, Ward 5b, and provided it with staff counselors. Through support groups, Shanti heard stories of PWAs being evicted from their homes or pressured to leave by their roommates. The idea of the Residence Program emerged from these conversations. It soon became a reality in 1983, through grant funding. Like much of Shanti’s work with PWAs in San Francisco, the Residence Program was another “first” —but not just in the city. It was also the first AIDS housing program in the United States.
Nurse Helen Schietinger had taken over Paul Dague’s position at the KS Clinic in 1982 and became familiar with Shanti there. The following year Shanti hired her to oversee the Residence Program. Schietinger designed the program with input from PWAs and modeled it on the principles of the disability rights independent-living movement, but she had great difficulty in securing a lease for long-term, low-cost flats for PWAs. Landlords, even gay landlords, were reluctant to lease to a high-profile group serving a villainized and feared group of people. Despite this, Shanti secured two homes and began the process of housing PWAs, with priority given to those most at risk of losing their homes or who lived on low incomes. Practical support volunteers helped paint and set up these homes prior to the residents’ move-in date and helped with their chores if they were too sick to work. Along with maintenance specialists, Shanti hired “resident advocates” who held monthly house meetings to hold support groups and check in with the house dynamics. Many Shanti residents would spend their final days in these homes, but the residences were not hospices. By the end of the 1980s, Shanti had more than ten residences in operation. With their addresses kept secret from those not affiliated with the program, these homes became communities. Through Shanti, PWAs were not only housed, they had a home.
The residence and hospital counseling programs influenced best practices of care for PWAs. Schietinger became an authority on AIDS home care. Addressing AIDS wasn’t just about the biological disease, or death. It was holistic, whole-person care. What is novel about Shanti’s work is the fact that services addressing feelings and emotions were considered on a par with having a person’s laundry done.
Shanti’s holistic response to the AIDS crisis was another step in the evolution of mutual aid. This approach cares about the whole person in one of their most vulnerable moments. The lesson for today from Shanti’s response resides in this fact. The transformative potential of mutual aid rests on proximity, as seen in Addams’ and Day’s work. With COVID-19, this closeness is now unfeasible for many reasons, but Shanti’s emphasis on presence does not rest on proximity. It is something that can be provided through a thoughtful phone call. Whether or not we choose to be holistic in our approach might be a deciding factor in the long-term effectiveness of these mobilizations.
Support JSTOR Daily! Join our new membership program on Patreon today.



