Maybe we should all just have a Morbidity and Mortality Weekly Report app, getting real-time updates of disease threats?


In 2018, a group of infectious disease experts reported on the emergence of human mpox in West and Central Africa from 1970 to 2017. At the time, they observed that “endemic human [mpox] has been reported from more countries in the past decade than during the previous 40 years.”
“Improving understanding of [mpox] will aid in developing innovative solutions to mitigate further spread of the virus,” the team suggested. “Furthermore, improved detection and response capacity for [mpox] will enhance capacity for responding to other zoonoses and orthopoxvirus events at regional and national levels.”
Is it now too late? On July 23, 2022, mpox was declared a global health emergency by the World Health Organization. The CDC is tracking US cases on this map.
Mpox is less fatal and less transmissible than the related smallpox, a global scourge which was declared eradicated in 1980. That’s good news, and so is the fact that the smallpox vaccine is also effective against mpox. Additionally, the vast majority of the people infected by the form of mpox now spreading can be expected to survive it.
However, there’s still serious cause for concern: children under eight are especially at risk, as is anyone with a compromised immune system. Those pregnant or breastfeeding are also at increased risk. For survivors, the disease is potentially disfiguring and can cause blindness because of corneal scarring. Complications like pulmonary distress and bronchopneumonia are also an issue. The effects of scapegoating and stigmatizing patients are harder to measure.
And because—as we’re all aware, thanks to COVID-19—viruses can mutate, especially when allowed to run unchecked through populations, this one could become a “more efficient human pathogen.”
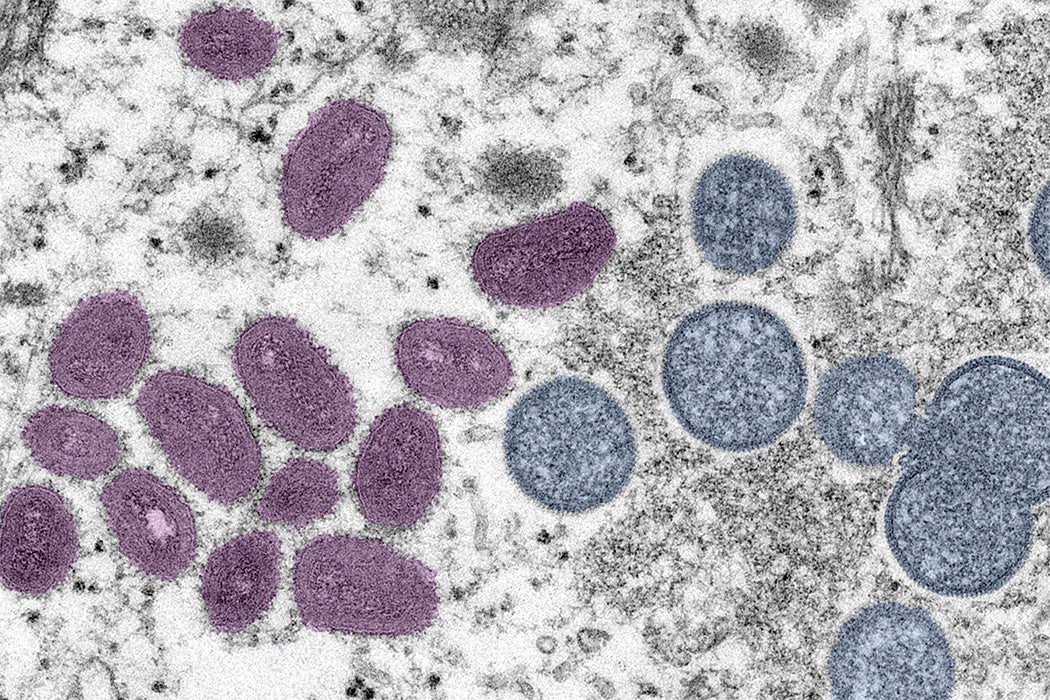
The original name of the disease, “monkeypox,” suggests its zoonotic origins: it was first seen in monkeys in 1958. Monkeys may not, however, have been the original source. Several other mammal species, especially rodents, are known to harbor the disease. It is considered to have jumped to humans around 1970. Human-to-human contact is spreading the disease today.
Weekly Newsletter
"*" indicates required fields
The original US outbreak in six Midwestern states in 2003 was caused by pet-to-human contact. This was traced to imported wild animals, who spread it to domesticated animals in the exotic pet trade. A team led by Gregory D. Huhn described the clinical characteristics of the thirty-four patients with confirmed cases, noting:
Five (15%) were defined as severely ill and 9 (26%) were hospitalized for >48 hr; no patients died. Previous smallpox vaccination was not associated with disease severity or hospitalization. Pediatric patients [under 18] were more likely to be hospitalized in an intensive care unit.
As with the COVID-19 pandemic, the US government’s response to the latest domestic outbreak has come under criticism. Notably, some 300,000 smallpox vaccine doses, held in reserve for potential acts of bioterrorism, went unused during the key early stages of the outbreak. And recently, New York City’s Health Commissioner called on the WHO to rename the virus, noting that, in the context of a “painful and racist history,” the name “monkeypox” had “potentially stigmatizing effects” on vulnerable communities. Most news agencies are now using the name “mpox” in their coverage of the disease.
Reports of cases at a Chicago jail and at least three colleges suggests this orthopoxvirus, one of a large family of similar diseases, may already be well on the loose.
Editor’s note: This story has been updated to reflect the preferred name for the disease.




_-_CDC.png){kind=link}