There’s been plenty of comparison between the coronavirus pandemic and its nineteenth century equivalents. But as the coronavirus pandemic transforms life around the world, one outcome in the U.S. has been a rise in hate crimes against Asian American people, especially following President Donald Trump’s use of the term “Chinese Virus” in his tweets and press briefings. “Chinese Virus” is an unwitting echo of the past, an echo of a time of cholera.


Across the U.S., Asian Americans are being attacked and harassed. Tellingly, it is in the language of ill hygiene that many of these incidents take place. In New York City, a man allegedly called an Asian woman “diseased” before physically attacking her. In Los Angeles, a man ranted at a Thai woman, accusing all Chinese people of being filthy. A number of articles have appeared (in sources of varying credibility) criticizing Chinese “wet markets” and traditional medicine practices, again assigning a kind of deeply cultural culpability for disease.
Weekly Newsletter
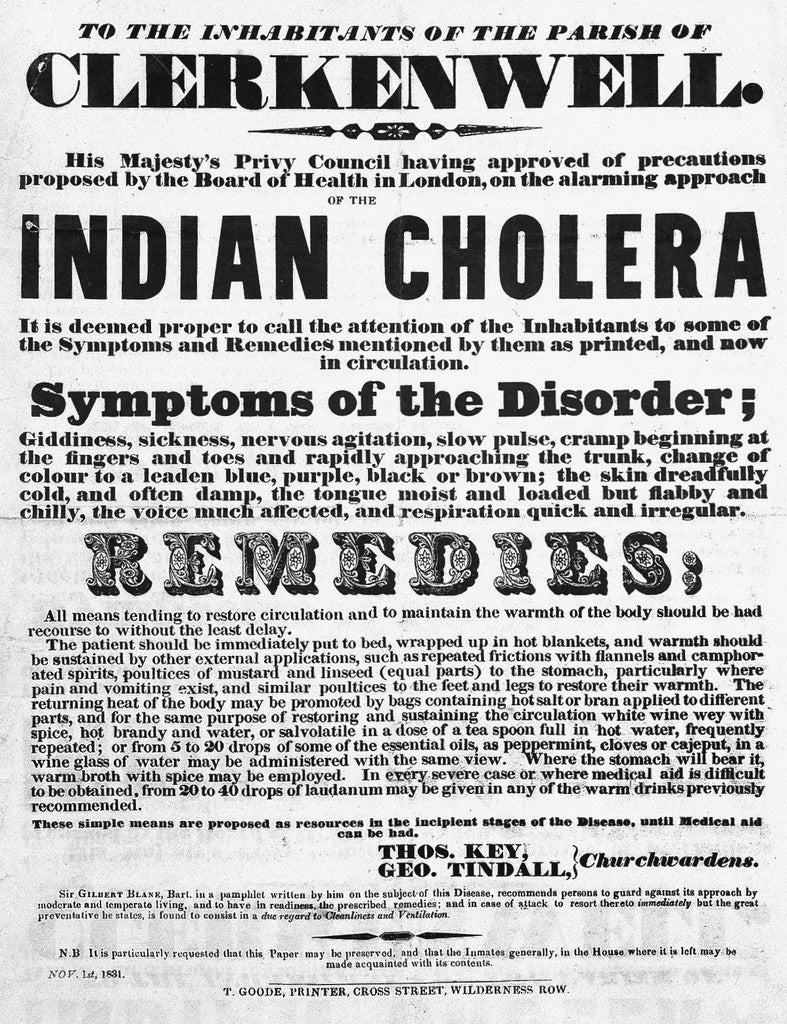
On March 4, 1884, Dr. Charles Macnamara delivered a lecture on “Asiatic Cholera” at the Westminster Hospital. Macnamara cited a government order from 1871 that read, “Asiatic cholera has a peculiar infectiousness of its own which, when local conditions assist, can operate with terrible force.” In the nineteenth century, “Asiatic Cholera” was used by Westerners to describe a new (to them) disease that originated in Bengal, India, and that was particularly virulent and deadly. The term was also used to define a whole subcontinent as diseased and unhygienic. South Asia was cast as being in some way to blame for a cholera that ravaged it just as seriously, if not more seriously, as it did Britain.

Historians mark the first cholera pandemic as beginning in 1817, spreading along trade routes from India to Myanmar, Sri Lanka, Thailand, Indonesia, China, and Japan by 1822. The second pandemic began in 1829, and the disease circulated from Britain to Canada, and from Mexico to Cuba. In this time, English-speaking doctors on both sides of the Atlantic referred to this “new” cholera by its place of origin. In 1831, the New York City Board of Health requested that “three of the City’s most prominent doctors be requested ‘to collect… with all possible speed, all information which can be obtained from Europe or Asia on the subject of the Oriental Cholera.’”
In the first waves of Asiatic Cholera, the British medical establishment was still deeply influenced by the humoral tradition that traced back to the writings of Galen. It was believed that disease stemmed from “miasmas” of bad air, especially in unsanitary conditions. In the first half of the nineteenth century, British doctors accepted some of the knowledge of Indian practitioners of Hindu Ayurveda or Muslim Unani. The commonly held belief was that it was the warm climate of India that exposed British soldiers to disease—an issue wealthier British colonizers avoided by sheltering in “hill stations” set on higher ground. Then, in 1854, a physician named John Snow proved that cholera was transmitted through water, and with this discovery, methods of responding to cholera changed drastically.
British understandings of sanitation, hygiene, and disease transmission advanced rapidly, but rather than leading to a common understanding that disease is an individual, not environmental phenomenon, British doctors began to deride Indian hygiene. As the historian David Arnold writes in the journal Past & Present:
The Indian origins of cholera and its almost global dissemination from Bengal made the disease a convenient symbol for much that the west feared or despised about a society so different from its own. One of the strongest expressions of this antipathy arose from the epidemiological connection between cholera and Hindu pilgrimage.
Existing fears about Indian society were paired with the anxiety that surrounded the potential advance of cholera. Arnold’s research shows that medical professionals, too, relied on moral judgments and broad generalizations in characterizing Indians on pilgrimage. The sanitary commissioner of Bengal, Dr. David Smith, wrote scathingly on disease and unsanitary conditions in the Hindu pilgrimage to the god Jagannath: “The human mind can scarcely sink lower than it has done in connection with the appalling degeneration of idol-worship at Pooree.”
By 1892, Dr. William Eggleston wrote in an article, “Oriental Pilgrimages and Cholera:”
The most riotous imagination could scarcely exaggerate the filth of India and Egypt and of the Hindoo and Mohammedan pilgrims, for when people use the same water for bathing, washing soiled clothes, and drinking, they are scarcely ripe for moral suasion. So long as the pilgrimages continue Europe and this country will be endangered and will be visited by cholera.
The British launched inquiries into the conditions of South Asian people on pilgrimages and ultimately classified pilgrims as a “dangerous class,” launching specific surveillance systems for pilgrims. This reveals the power of the “colonial gaze:” the ability to categorize whole practices, such as Hindu or Muslim pilgrimage, as senseless and backwards.
David Arnold (the historian) closes his illuminating work on “Cholera and Colonialism in British India,” like this:
Like any disease, cholera has in itself no meaning: it is only a micro-organism. It acquires meaning and significance from its human context.
In the British Empire in the nineteenth century, cholera was used to drive a wedge between cultures, even as British doctors improved their understanding of disease transmission and moved to a new era of medical science. Between fear of cholera and ignorance of pilgrimage practices, the British medical establishment characterized a whole culture as filthy and insensible.
We should learn from, instead of repeating, the racist assignations of the past.