An estimated one to two percent of the human population is born intersex, with variations of “genitals, chromosomes or reproductive organs that don’t fit into a male/female sex binary.” These variations—there are some forty different named ones—may be present at birth or develop later. Such random, natural human differences have in the past, and in some cases still are, framed as medical problems in need of correction.


Intersexuality has been called a disorder—some prefer divergence or difference—of sexual development (DSD). The idea that intersex is a “disorder” has been challenged by intersex activists, who note that only a few generations ago homosexuality was considered a medical/psychological disorder. The Cleveland Clinic’s definition of intersex, quoted in the first sentence, goes on to say that “being intersex isn’t a disorder, disease or condition.”
As historian Sandra Eder writes, even the “nomenclature is quite contested.” “Nonbinary gender,” “third sex,” and “two-sex being” have been suggested as alternatives to intersex. Some intersex activists have decried outdated terms like “hermaphrodites” and “Zwitter” (from the German for hybrid or hermaphrodite), while other activists have worked to reclaim these terms as a form of in-group pride. In the 1950s, the period Eder explores with her research, “intersexes,” “intersexuality,” “hermaphroditism,” and “pseudo-hermaphroditism” were all used.
In the 1950s, however, intersex infants and children were definitely viewed as a biomedical problem. “Sex roles”—the telling phrase contains its own critique—were supposedly hard and fast, and anomalies needed to be fixed. This was the era that established “surgical genital normalization,” the surgical process of making a child’s genitals “fit” a chosen sex for what was called “optimum gender of rearing.” The intervention sought to make each “abnormal” child’s body fit a “normal” gender identity by surgically changing the genitalia and/or removing hormone-producing organs.
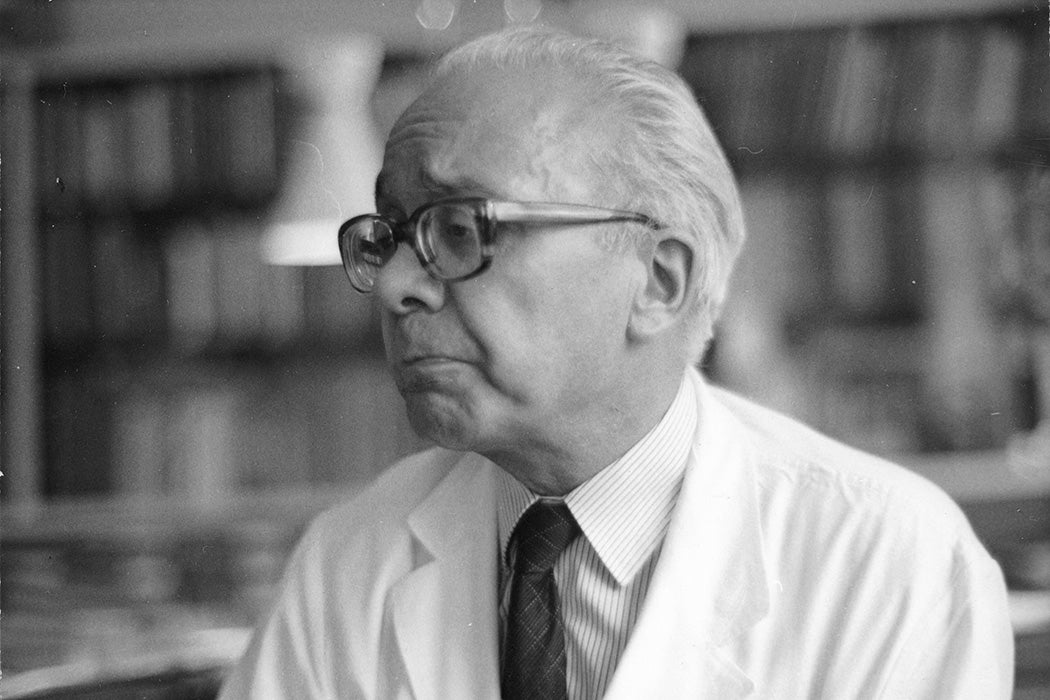
Eder details the transatlantic process that consolidated and standardized modern intersex case management. Her main players are Lawson Wilkins and John Money at Johns Hopkins in Baltimore and Andrea Prader at the University Children’s Hospital in Zurich, Switzerland. The resulting protocols “would shape the lives of intersex patients for more than six decades,” she writes. The collaboration across oceans set up “a host of evolving recommendations on what sex to choose for so-called hermaphroditic children, if and when to change a child’s sex, what information to share with patients, and how to evaluate behavior and treatment success.”
In addition, the 1950s gave birth to a “new diagnostic category—the concept of a person’s gender role.” As Eder notes, “many scholars see [this] as the first formulation of a social gender distinct from a biological sex.” The idea that gender is a social construct thus emerged alongside the fact that gender could be quite literally created, surgically and hormonally.
Weekly Newsletter
What emerged was a “determination within the medical community to normalize the bodies of those who transgress the two-sex binary.” “Normalize” is of course a loaded word: what’s normal statistically is always accompanied by outliers; the definition of the outlines can be heavily ideological. Eder notes that scholarship now “emphasizes that this treatment regime has caused immense suffering through irreversible nonconsensual surgery.”
Eder continues, “since the late 1980s patient activism and critical scholarship have played a major role in challenging [surgical genital normalization’s] hitherto unquestioned predominance.” In 2015, Malta became the first country to ban “unnecessary surgeries on children with sex variations”; Germany, Greece, Iceland, Spain, and Portugal have since followed with similar laws, while some fifty countries signed a UN statement on measures to protect intersex people. While some US states have banned gender-affirming surgeries, none seem to have banned infant intersex surgeries. In 2020, the Lurie Children’s Hospital in Chicago apologized for its history of infant intersex surgeries, calling it “harmful and wrong.”


_AB.2.55_Prader.jpg){kind=link}